

Clinically meaningful improvements over standard care were observed in both first and second line, as reported in the MARIPOSA and MARIPOSA-2 phase III trials
Resistance inevitably emerges in most patients with EGFR-mutated (ex19del or L858R) advanced non-small-cell lung cancer (NSCLC) treated with the third-generation EGFR TKI, osimertinib (Ther Adv Med Oncol. 2022;14:17588359221144099) and there remains an unmet need for new first-line treatments and options following relapse. Presentations in a Presidential Symposium at the ESMO Congress 2023 (Madrid, 20–24 October) revealed positive findings with the EGFR-MET bispecific antibody, amivantamab, given as combination therapy in two highly awaited phase III trials – MARIPOSA in treatment-naïve patients (LBA14) and MARIPOSA-2 in the osimertinib-relapsed setting (LBA15) – confirming promising previous reports from the CHRYSALIS and CHRYSALIS-2 studies (J Clin Oncol. 2023;41:16_suppl:9134; J Clin Oncol. 2022;40:16_suppl:9006).
In the MARIPOSA trial, the risk of disease progression or death was reduced by 30% in 429 patients who received amivantamab combined with a brain-penetrant irreversible third-generation EGFR TKI, lazertinib, compared with 429 patients on osimertinib monotherapy (hazard ratio [HR] 0.70; 95% confidence interval [CI] 0.58–0.85; p<0.001), with a median progression-free survival (PFS) of 23.7 months (95% CI 19.1–27.7) and 16.6 months (95% CI 14.8–18.5), respectively, at a median follow-up of 22.0 months (LBA14). Objective response rates (ORR) were similar with amivantamab–lazertinib (86%) and osimertinib (85%), but with longer median duration of response among confirmed responders on amivantamab-lazertinib: 25.8 months (95% CI 20.1–not estimable) versus 16.8 months (95% CI 14.8–18.5) with osimertinib. In an interim overall survival (OS) analysis, there was a favourable trend for amivantamab–lazertinib over osimertinib (HR 0.80; 95% CI 0.61–1.05; p=0.11). The incidence of most EGFR- and MET-related adverse events (AEs) was higher with amivantamab–lazertinib than with osimertinib. Treatment-related adverse events (TRAEs) leading to discontinuations of all agents occurred in 10% of patients treated with amivantamab plus lazertinib and 3% with osimertinib. Any venous thromboembolism (VTE) occurred in 37% of patients in the amivantamab–lazertinib group and 9% on osimertinib, leading the investigators to recommend prophylactic anticoagulation for the first 4 months of treatment in ongoing trials of amivantamab–lazertinib.
Commenting on the findings, Prof. Zofia Piotrowska from the Massachusetts General Hospital/Harvard Medical School, Boston, MA, USA, says, “The combination showed clinically meaningful PFS improvements over the current standard of care, although we have to weigh the benefits against the increased toxicities associated with two drugs and the practicalities of adding intravenous amivantamab requiring biweekly administration to an oral regimen. In particular, dermatological toxicities, such as paronychia and rash, were more common with the combination. Even though they were primarily low grade, these side-effects may impact patients’ quality of life, particularly given the long duration of treatment, and clinicians will need to weigh these risks against the degree of clinical benefit when considering this regimen.”
In the second-line setting, in the MARIPOSA-2 trial, PFS was significantly improved in patients receiving amivantamab–chemotherapy (n=131; HR 0.48; 95% CI 0.36–0.64; p<0.001) and amivantamab–lazertinib–chemotherapy (n=263; HR 0.44; 95% CI 0.35–0.56; p<0.001) versus chemotherapy alone (n=263; median PFS of 6.3 months and 8.3 months versus 4.2 months, respectively) at a median of 8.7 months of follow-up (LBA15).
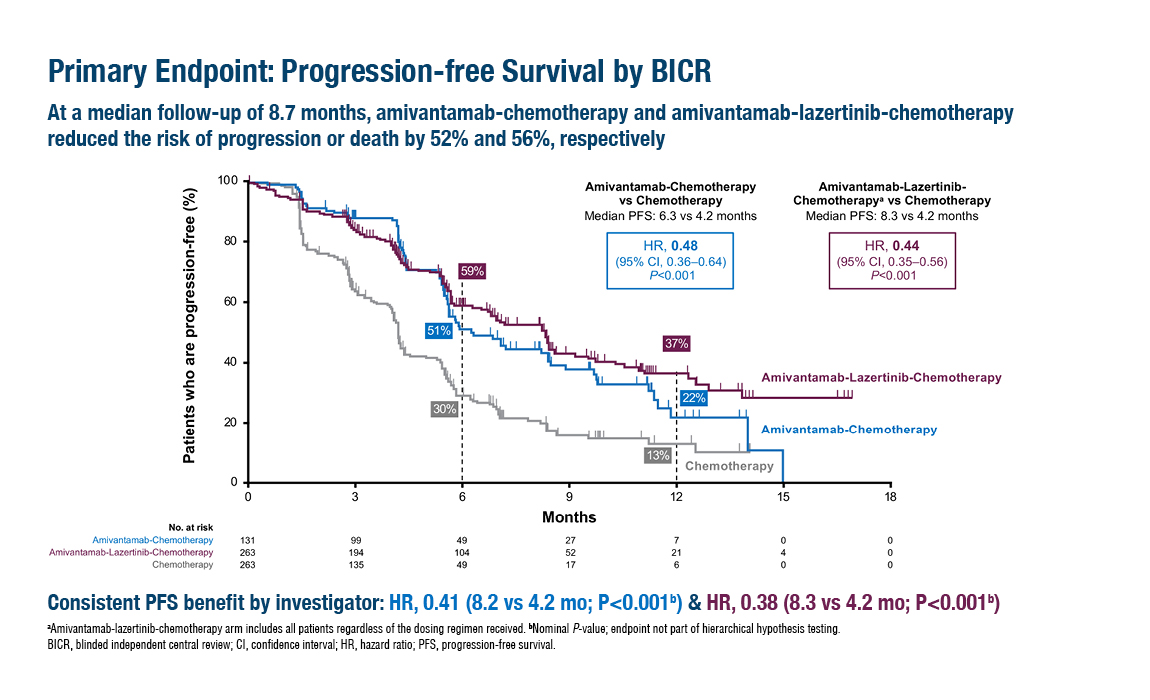
Figure. Median PFS was significantly longer with amivantamab–chemotherapy and amivantamab–lazertinib–chemotherapy than with chemotherapy alone in the MARIPOSA-2 trial (ESMO Congress 2023, LBA15)
The ORR was 64% for amivantamab–chemotherapy and 63% for amivantamab–lazertinib–chemotherapy versus 36% for chemotherapy (p<0.001 for both). OS data are immature, but interim analysis demonstrated an HR of 0.77 (95% CI 0.49–1.21) for amivantamab–chemotherapy versus chemotherapy and an HR of 0.96 (95% CI 0.67–1.35) for amivantamab–lazertinib–chemotherapy versus chemotherapy. Median intracranial PFS was 12.5 months for amivantamab–chemotherapy and 12.8 months for amivantamab–lazertinib–chemotherapy versus 8.3 months for chemotherapy (HRs of 0.55 and 0.58; p=0.001 and p<0.001, respectively). Grade ≥3 haematological toxicity was common with the triple combination, namely, neutropenia (55%), thrombocytopenia (37%) and leukopenia (27%), which necessitated a dosing schedule change. In the amivantamab–chemotherapy group, the most common grade ≥3 AEs were neutropenia (45%), leukopenia (20%) and thrombocytopenia (15%).
“It appears, based on these data, that combinations adding amivantamab and amivantamab/lazertinib to chemotherapy lead to clinically meaningful improvements in PFS and ORR over our current standard of care, but come at the cost of increased toxicities. The improvements in intracranial PFS in particular are encouraging, as we have limited treatment options for patients with CNS progression on osimertinib, but the added risks will need to be considered carefully when selecting patients who may benefit from this approach,” continues Piotrowska. The study findings confirm the efficacy of the combination of amivantamab plus chemotherapy seen in the PAPILLON trial in advanced NSCLC and EGFR exon 20 insertion mutations also presented at the ESMO Congress 2023.
For EGFR-mutated (ex19del or L858R) NSCLC, Piotrowska emphasises that the results of the MARIPOSA trials must be put into context with each other and with other new data, including findings from the FLAURA2 trial (NCT04035486) presented at the 2023 World Conference on Lung Cancer. “Instead of looking at each trial individually, a broad view of the treatment landscape is now needed, considering the various available options and the optimal sequence, which may not be the same for every patient. If we use amivantamab–lazertinib in the first-line setting as in MARIPOSA, then the combination in MARIPOSA-2 will not be appropriate after relapse. For example, we may choose to use the approved osimertinib regimen in the first line, with or without chemotherapy, then consider an amivantamab combination second line.”
Further investigations of resistance mechanisms may provide information on biomarkers that can guide clinical decision making and may aid in the development of more new treatments. The ongoing phase II SAVANNAH study is evaluating the combination of osimertinib with the selective MET TKI, savolitinib, in patients with MET-mediated resistance to osimertinib (NCT03778229), while the phase III SAFFRON trial is investigating osimertinib–savolitinib versus platinum-doublet chemotherapy in the same patient population (NCT05261399). Piotrowska also points to new fourth-generation TKIs that target resistance mediated by EGFR C797S as an alternative direction to improve on the success of osimertinib and highlights the development of antibody–drug conjugates, such as patritumab deruxtecan, as another interesting avenue following progression on EGFR TKI treatment. “The complexity of treating EGFR-mutated NSCLC increases as exciting new trial data are published, but expanding available treatment options can only be a good thing for our patients,” concludes Piotrowska.
Abstracts discussed:
Cho BC, et al. Amivantamab plus lazertinib vs osimertinib as first-line treatment in patients with EGFR-mutated, advanced non-small cell lung cancer (NSCLC): Primary results from MARIPOSA, a phase III, global, randomized, controlled trial. ESMO Congress 2023, LBA14
Presidential Symposium 3, 23.10.2023, h. 16:30 – 18:15, Madrid Auditorium – Hall 6
Passaro A, et al. Amivantamab plus chemotherapy (with or without lazertinib) vs chemotherapy in EGFR-mutated advanced NSCLC after progression on osimertinib: MARIPOSA-2, a phase III, global, randomized, controlled trial. ESMO Congress 2023, LBA15
Presidential Symposium 3, 23.10.2023, h. 16:30 – 18:15, Madrid Auditorium – Hall 6




