An analysis of the BEATcc trial showed that PD-L1 is not a robust biomarker for response to treatment
Adding atezolizumab to chemotherapy and bevacizumab has previously been demonstrated to improve progression-free survival (PFS) and overall survival (OS) in patients with untreated recurrent/metastatic cervical cancer in the phase III BEATcc trial (Lancet. 2024;403:31–43). A post-hoc analysis of the trial, presented at the ESMO Gynaecological Cancers Congress 2025 (Vienna, 19–21 June), investigated effects according to PD-L1 status and found similar PFS benefits either in patients with a PD-L1 combined positive score (CPS) ≥1 (hazard ratio [HR] 0.54; 95% confidence interval [CI] 0.39–0.74) or in those with a PD-L1 CPS <1 (HR 0.48; 95% CI 0.28–0.82) (Abstract 10O). Hence, there was no predictive effect of CPS for PFS (interaction p=0.73). The analysis was conducted at a median follow-up of 32.8 months in 313 patients of whom around 70% had CPS ≥1.
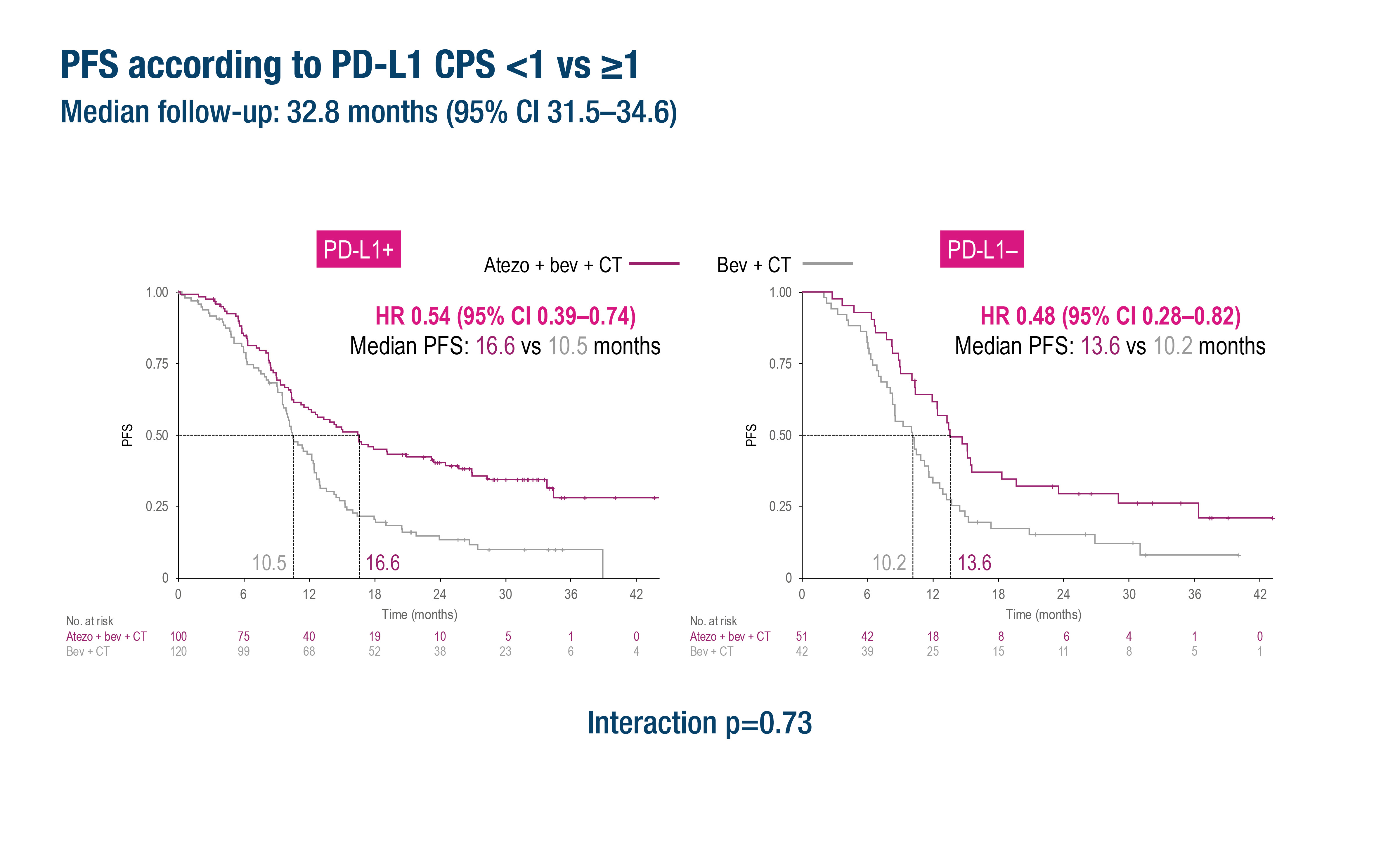
Figure. The addition of atezolizumab to chemotherapy and bevacizumab had similar effects on PFS regardless of PD-L1 CPS (≥1 versus <1) status in the BEATcc trial in patients with untreated recurrent/metastatic cervical cancer (ESMO Gynaecological Cancers Congress 2025, Abstract 10O)
Similar findings were observed for PFS2 (time from randomisation to second progression or death), where median values were 23.3 months and 24.3 months with atezolizumab plus chemotherapy and bevacizumab in patients with CPS ≥1 and <1, respectively (interaction p=0.53). In an interim analysis, median OS was 33.2 months in patients with CPS ≥1 and 37.3 months in patients with CPS <1 (interaction p=0.12). Final OS results are awaited.
Commenting on the findings, Prof. Christian Marth from the Medical University of Innsbruck, Austria, says: “The BEATcc trial confirms the findings of the KEYNOTE-826 trial, which showed survival advantages when pembrolizumab was added to chemotherapy with or without bevacizumab in patients with CPS ≥1 (N Engl J Med. 2021;385:1856–1867). Conducting the BEATcc trial by including bevacizumab for all patients and demonstrating consistently impressive PFS is an important step forward and means that we could now consider immunotherapy in combination with bevacizumab regardless of PD-L1 status.”
He highlights the apparent immunogenicity of cervical cancer and how immunotherapy is being used in earlier settings but notes, “Nowadays, some patients in the metastatic setting might already have received immunotherapy earlier in their disease course. Further studies are needed to understand whether immunotherapy could be used again at progression.”
Marth concludes by suggesting potential new ways to build on current immunotherapy success: “Bispecific immunotherapy could be a step up and also combining immunotherapy with antibody–drug conjugates, such as tisotumab vedotin that has shown later-line activity (N Engl J Med. 2024;391:44–55), may help progress to continue.”
Programme details
De Giorgi U, et al. Efficacy according to PD-L1 status in the BEATcc (ENGOT-Cx10/GEICO 68-C/JGOG1084/GOG-3030) randomised phase III trial of first-line atezolizumab (atezo), chemotherapy (CT) and bevacizumab (bev) for metastatic, persistent or recurrent cervical cancer (R/M CC). ESMO Gynaecological Cancers Congress 2025, Abstract 10O
Proffered Paper Session, 19.06.2025, h. 14:00 – 15:30, Hall D